At Gartside Street Dental Lounge in Manchester city centre, our clinicians share practical guidance to help you make confident treatment decisions.
"I’d rather have a root canal" became the punchline of dental jokes for a reason. Root canal treatment carries the worst reputation of any procedure in dentistry, partly fairly and partly very unfairly. The reality is that most of the pain people associate with root canals is actually the pain of the abscess that brought them to the dentist in the first place — the treatment itself, performed under modern conditions, feels far closer to a deep filling than to the horror story most people imagine. This post explains what root canal treatment actually involves, what it feels like, and why saving the tooth is almost always preferable to losing it.
A quick anatomy lesson first, because the jargon makes the procedure sound worse than it is. Inside every tooth is a hollow space called the pulp, which contains the nerve and the blood vessels that nourished the tooth as it grew. The pulp runs down through narrow channels in the roots called the root canals. When the pulp gets infected — usually because deep decay has reached it, or because the tooth has been cracked or traumatised — it begins to die, and the body responds with inflammation. The infected pulp is a closed system with nowhere to drain, so pressure builds and the result is the characteristic toothache: a deep, throbbing, often unbearable pain that sometimes radiates to the ear or jaw.
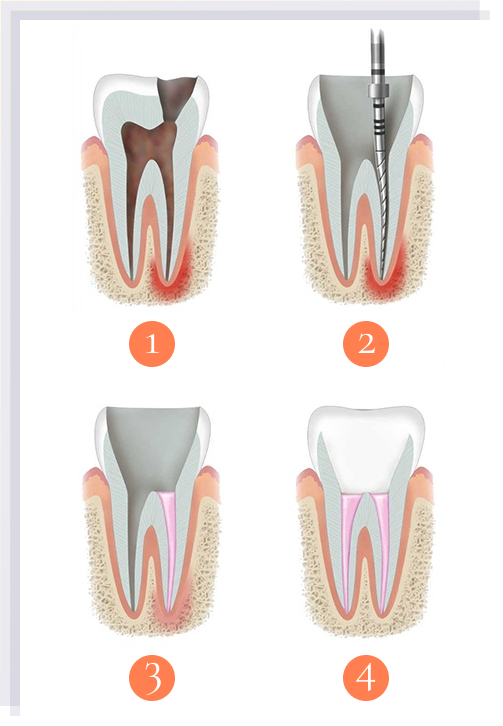
Root canal treatment is the procedure that addresses this. We numb the tooth thoroughly, isolate it under a rubber dam (a thin sheet that keeps the tooth dry and clean), open the top of the tooth to reach the pulp chamber, remove the infected pulp, clean and shape the inside of the root canals, and seal them with a rubber-like material called gutta-percha. The tooth is then restored with a filling and, in most cases, a crown to protect it long-term.
What it actually feels like, honestly, under modern anaesthetic. Once you are properly numb — and tooth numbing is usually thorough for root canals — the procedure feels very similar to having a deep filling. You feel the rubber dam, the pressure of the instruments, the sound of the small motor turning the files, and water spraying into the tooth. You should not feel sharp pain. If at any point you do, you raise your hand and we top up the anaesthetic. Infected teeth are sometimes harder to numb because inflammation reduces the effectiveness of local anaesthetic, so top-ups are normal and not a sign that anything has gone wrong.
Several modern tools have transformed how root canals are done compared with twenty years ago. Rotary nickel-titanium files spinning in an electric handpiece have replaced laborious hand-filing, dramatically reducing appointment time and improving the consistency of cleaning. Apex locators — small electronic devices — measure the exact length of each root, replacing the multiple X-rays that used to be needed to confirm working length. Operating microscopes magnify the inside of the tooth so we can see canals and detail that the naked eye misses entirely. Modern irrigation protocols use a sequence of antibacterial solutions to clean the canals more thoroughly than old saline rinses ever did.
Success rates have improved as a result. With modern technique, root canals on teeth with relatively straight roots — front teeth and most premolars — succeed in around 90 to 95 per cent of cases at five-year follow-up. Molars with curved or complex root anatomy succeed in around 85 to 90 per cent. When failures do occur, retreatment is often possible, either by repeating the root canal or by surgical apicectomy at the root tip. We refer to a specialist endodontist for complex cases.
A typical treatment day looks like this. Initial diagnosis with X-rays and clinical testing. Local anaesthetic, with topical gel applied first. Rubber dam placed over the tooth to keep the field clean and isolate the tooth from saliva. The pulp chamber is opened with a small drill. Each root canal is identified, measured, and cleaned with rotary files under irrigation. A temporary filling is placed if treatment is being completed across two visits, or the canals are sealed and the tooth is restored if completed in a single visit. The whole appointment usually takes one to two hours per session, depending on the tooth.
Single-visit versus two-visit treatment. Many root canals are now completed in one extended visit, which is more comfortable for patients than splitting the work and reduces the risk of bacteria recolonising the canals between appointments. Some teeth — particularly those with active acute infection or persistent symptoms — benefit from a two-visit approach with an antibacterial dressing left inside the tooth for one to two weeks. Your dentist will explain which is appropriate for your tooth.
What to expect afterwards. The infection-related pain — the abscess pain that probably brought you in — usually starts to ease within twenty-four to forty-eight hours of treatment, often dramatically. Some tenderness in the tooth and surrounding gum is normal for three to seven days, well managed by alternating paracetamol and ibuprofen at recommended doses. The tooth may feel mildly bruised when biting on it for a couple of weeks. Anything beyond that — sustained pain, increasing swelling, fever, or persistent throbbing — warrants a call.
Why a crown often follows. Root-canalled teeth are mechanically weaker than living teeth. Removing the pulp and creating an access opening reduces the structural integrity of the tooth, and back teeth in particular take heavy chewing forces. Without protection, an unrestored root-canalled molar has a meaningful risk of fracturing — sometimes catastrophically — within a few years. A crown placed within a few months of the root canal protects the tooth and substantially extends its lifespan. For some front teeth a smaller bonded restoration is sufficient, but molars almost always benefit from a crown.
The alternative to root canal is extraction. Removing the tooth is faster, cheaper short-term, and final. The downside is that the gap left behind affects the bite, the adjacent teeth, and often the appearance of your smile. The gap then usually needs to be filled with an implant, a bridge, or a denture, all of which are more expensive and more invasive than the root canal would have been. Saving the natural tooth is almost always preferable when feasible — your own tooth, retained, is the gold standard. When is root canal treatment not possible? Severely cracked teeth with vertical fractures running into the root are usually unsalvageable. Teeth with insufficient remaining structure to support a future crown are sometimes better extracted. Teeth in advanced periodontal disease with major bone loss have a poor long-term prognosis even with successful root canal. In these cases extraction and replacement is the right call rather than throwing good money at a tooth with a poor outlook. We will tell you honestly when this applies.
When previous root canals fail — which happens in around five to fifteen per cent of cases over time — retreatment by an endodontic specialist is usually possible. The original sealing material is removed, the canals are cleaned again, and the tooth is resealed. Success rates for retreatment are lower than for initial treatment but still good for most cases.
How to recognise that you might need one. Severe lingering toothache, particularly after exposure to hot or cold. Spontaneous pain that wakes you at night. A pimple-like swelling on the gum near a tooth, often draining yellowish fluid. A tooth that has darkened compared with its neighbours. Pain on biting that has been worsening over weeks. Any of these warrant prompt assessment. Untreated dental infection can spread, and although serious systemic complications are rare in healthy adults, they do happen. Earlier diagnosis is better both for your comfort and for the success rate of treatment.
Cost realism. UK private root canal treatment varies by tooth and complexity — front teeth are simpler, molars more complex. Roughly £400 to £700 for an anterior tooth, £700 to £1,200 for a molar with multiple curved roots. A crown afterwards is an additional £700 to £1,200 depending on material. Total cost is usually less than the cost of an extraction followed by an implant, and much less than the cost of multiple problems that develop from a missing tooth left untreated.
If you have a tooth you have been ignoring because you fear it might need a root canal, the chances are that the procedure itself is far less unpleasant than the abscess that is coming if you wait. Earlier diagnosis is better for you and for the tooth. Book a consultation and we will assess the tooth honestly and explain your options. Ready to Transform Your Smile?
Take the first step towards your dream smile. Book a free consultation with our expert team at our Manchester clinic and discover how we can help you achieve the confidence you deserve.